This is an E log book to discuss our patients de identified health data shared after guardians informed consent.
Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve this patients clinical problems with collective current best evidence based inputs.
This E-book also reflects my patients centered online learning portfolio and your valuable comments in comment box are most welcome.
I have been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency and to comprehend clinical data including history, clinical finding investigations and come up with a diagnosis and treatment plan.
CHIEF COMPLAINTS
- Fever since 3 days
- cough (dry cough) since 3days
- shortness of breath grade 4 since 3 hours
HISTORY OF PRESENTING ILLNESS
Patient was apparently asymptomatic 3 days ago then he had fever associated with chills and rigors then he developed dry cough, and then developed SOB Grade 4 since 3 hours.
No h/o cold, nausea, vomiting, loose stools.
PAST HISTORY
Not a known case of Diabetes, Hypertension, Tb, Asthma, Epilepsy, CAD, Chemotherapy
FAMILY HISTORY
Not significant
PERSONAL HISTORY
Diet - mixed
Appetite - Decreased
Bowel and bladder - adequate
Allergies -no
Addiction - intake of alcohol
90ml daily
GENERAL EXAMINATION
The patient is conscious, coherent, cooperative, well oriented to time, place and person
Thin built and malnourished
The patient was examined after taking consent in a well lit room.
Vitals
Temperature : Afebrile
Pulse: 90
BP:120/70 mm/ hg
RR :26
SPO2 : 92%
GRBS:127 MG%
Pallor : ABSENT
Icterus : ABSENT
Clubbing :ABSENT
Cyanosis :absent
Lymphadenopathy: absent
Pedal edema: absent
SYSTEMIC EXAMINATION
CVS
Apex beat 6 th intercoastal space
No thrills
S1 S2 heard
No murmurs
ABDOMEN EXAMINATION
RESPIRATORY SYSTEM
dyspnoea wheeze+
Central trachea
Bilateral air entry +
Bilateral basal crepts +
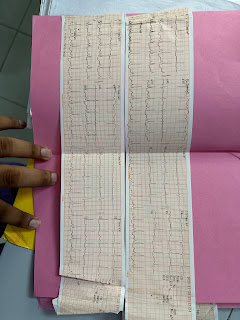
INVESTIGATIONS














Comments
Post a Comment