13 yr old with auto immune
This is an E log book to discuss our patients de identified health data shared after guardians informed consent.
Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve this patients clinical problems with collective current best evidence based inputs.
This E-book also reflects my patients centered online learning portfolio and your valuable comments in comment box are most welcome.
I have been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency and to comprehend clinical data including history, clinical finding investigations and come up with a diagnosis and treatment plan.
A 13 year old female student came to the opd with
CHIEF COMPLAINTS:
- Shortness of breath since 4 days
- Vomitings since 2 days
HISTORY OF PRESENTING ILLNESS
Patient was apparently asymptomatic till the age off 11 that is in 2020, she pursued her studies residing in a hostel where she noticed development of multiple neck swellings which were bilateral and also had a complaint of cough and fever which were on and off. For which she was referred to the RMP.
Since she has a mother with a history of tuberculosis, she was initiated with ADT which she followed for two months starting from 2021 June after which she developed a fever so the ADT was stopped and was referred to Hyderabad.
In Hyderabad, the patient was evaluated for cough but none of the investigations showed AFB.
In the same period she developed wrist joint pains and knee paints, for this there was a suspicion that it might be an autoimmune disease and was started on the tablet wyslone and HCQ which she used for 15 days and stopped.
Later she again developed joint pains, facial puffiness, pedal oedema, fever and cough.
In the same period, lymph node biopsy was done (report unavailable), GeneXpert showed rifampicin resistant TB.
ANA profile positive for dsDNA.
So she was initiated on ADT empirically on may 2022. Before starting ADT, she noticed facial rash and hair loss. Now she has come with history of SOB ( grade 2-3) and vomiting which were non projectile, non bilious, 4 episodes till date containing ingested food as content.
PAST HISTORY
Not a known case of Diabetes, hypertension, epilepsy, CAD, asthma
NATAL HISTORY
Second degree consanguinity present.
She was a first child born in 201o, LSCS delivery.
Immunization history unknown to the father.
FAMILY HISTORY
Mother was a known case of tuberculosis, diagnosed in 2014. She died in 2022 September ( did not use ADT regularly )
PERSONAL HISTORY
Diet: mixed
Appetite: decreased
Bladder: urine reduced
Sleep: adequate
No addictions
TREATMENT HISTORY
Used ADT for 6 months then discontinued
GENERAL EXAMINATION
Patient is consious, coherent, cooperative, well oriented to time, place and person. Moderately built and moderately nourished.
Pallor present

Edema present in the lower limb which was of pitting type

No cyanosis, icterus, clubbing, lymphadenopathy
VITALS
Temperature: 98.4 F
PR: 126 bpm
BP: 130/90 mmHg
RR: 26 cpm
Sp02: 98%
SYSTEMIC EXAMINATION
Patient is examined in a well lit room, in the sitting position.
RESPIRATORY SYSTEM:
BAE (+)
Vocal resonance reduced in affected areas
Dull note in affected areas
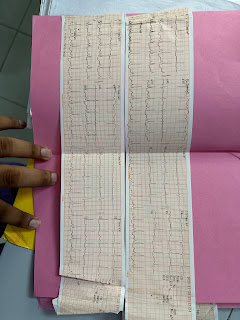
CARDIOVASCULAR SYSTEM
S1, S2 heard
Pericardial rub heard
No murmurs
PER ABDOMEN
Free fluid present
Tenderness in right and left hypochondria and epigastrium
CNS
Higher mental state:
Consious, coherent, cooperative, well oriented to time place and person.
Cranial nerve examinations: normal
Motor system:
RT LT
Biceps ++ ++
Triceps 2+ 2+
Supinator + +
Knee 2+ 2+
Ankle + +
CLINICAL IMAGES


INVESTIGATIONS
|
HAEMOGLOBIN |
# 6.8 gm/dl |
|
TOTAL COUNT |
5,400 cells/cumm |
|
NEUTROPHILS |
62% |
|
LYMPHOCYTES |
34% |
|
EOSINOPHILS |
1% |
|
MONOCYTES |
3% |
|
BASOPHILS |
0% |
|
PCV |
# 23.3 vol % |
|
MC V |
# 77 4 fl |
|
MC H |
# 22.6 pg |
|
MCH C |
# 29.2 % |
|
RDW-CV |
# 20.1 % |
|
RDW-SD |
57.8 fl |
|
RBC COUNT |
# 3.01 millions/cumm |
|
PLATELET |
1.20 lakhs/cu.mm |

8. USG findings:
|
1. FLUID RESTRICTION LESS THAN 1.5L/DAY |
|
|
|
2. SALT RESTRICTION LESS THAN 1.2GM/DAY |
|
|
|
3. INJ. LASIX 40 MG IV/BD |
|
|
|
4. INJ. METHYLPREDNISOLONE 250 MG IN 100ML NS IV/OD |
|
|
|
5. TAB. ALDACTONE 25MG PO/OD |
|
|
|
6. TAB. SHELCAL 500 MG PO/OD |
|
|
|
7 VITALS MONITORING |
 |




Previously used tuberculoid drug



Comments
Post a Comment