A 56 year old with shock secondary to sepsis UTI
This is an a online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
The patient/ attender was informed the purpose of the information being acquired. An informed consent was taken from patient/ attender and there is omission of information that was requested to be omitted.
CONSENT WAS GIVEN BY BOTH PATIENT AND ATTENDERS
Case presentation
Patient was bought to the casualty with the complaint of
Altered sensorium since 2 days
Decreased urine output since 2 days
Shortness of breath since 1 day
History of presenting illness
Pt was apparently asymptomatic 2 days back then he developed decreased urine output .
Foleys catherization was done outside, patient pulled the foleys catheter which caused urethral rupture .later catheterisation was done under cystoscope guidance . Altered sensorium since 2 days, irritable behaviour, not able to identify attenders , shortness of breath since 1 day insidious in onset and gradually progressive ( grade 1- grade 3)
No h/o Orthopnea
No h/o fever,vomitings loose stools , pain abdomen
Past history-
K/c/o type 2 DM , and HTN since 7 years ( on unknown medication )
DIET: MIXED
SLEEP: ADEQUATE
BOWEL: REGULAR
BLADDER: DECREASED MICTURATION
NO ALLERGIES
ADDICTIONS - ALCOHOL 90ml twice or thrice in a WEEK since
FAMILY HISTORY:
NO H/O SIMILAR COMPLAINTS IN THE FAMILY
THE PATIENT IS CONSCIOUS, COHERENT, COOPERATIVE
MODERATELY BUILT AND NOURISHED
NO SIGNS OF ICTERUS ,CYANOSIS, CLULBBING of fingers , EDEMA of feet ( non pitting )
VITALS:
TEMP: AFEBRILE
PR: 94BPM
RR: 36 CPM
BP: 90/60 MM HG
SPO2: 95% @ RA
GRBS: 95 MG/DL
RS: BAE+, NVBS
TRACHEA: CENTRAL
NO DYSPNOEA AND WHEEZE
NO RHONCHI
CNS:
LEVEL OF CONSCIOUSNESS: CONSCIOUS, ALERT
SPEECH: SLURRED
NECK STIFFNESS ABSENT
KERNINGS SIGN ABSENT
CRANIAL NERVES: NORMAL
MOTOR SYSTEM: NORMAL
SENSORY SYSTEM: NORMAL
GCS: 15/15 E4V5M6
TONE:
UL: NORMAL
LL: NORMAL
POWER:
UL: BOTH 4/5
LL: BOTH 4/5
REFLEXES: RT LT
B: +2 +2
T: +2 +2
S: +1 +1
K: +2 +2
A: +2 +2
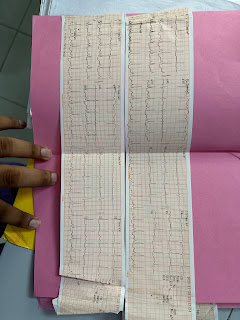
INVESTIGATIONS
HB 9.5
TLC 6300
PCV 27.1
MCV 63.1
PLT 18000
TB 6.54
DB 5.33
UREA 99
CREATININE- 3.5
NA- 135
K -4.8
Magnesium-2.0
PROVISIONAL DIAGNOSIS
SHOCK SECONDARY TO SEPSIS UTI
TREATMENT
IV FLUIDS NS BOLUS
INJ MEROPENIUM
INJ LINEZOLID
INJ OPTINEURON
INJ SOD BICARBONATE


Comments
Post a Comment