A 65 YEAR OLD MALE WITH HEART FAILURE
This is an online e-log book to discuss our patient de-identified health data shared after taking his / her / guardian's signed informed consent. Here we discuss our individual patients' problems through a series of inputs from the available global online community of experts with an aim to solve those patients' clinical problems with collective current best evidence-based information.
This E blog also reflects my patient-centered online learning portfolio and your valuable input in the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and coming up with diagnosis and treatment plans. is an online e-log book to discuss our patient's de-identified health data shared after taking his / her / guardians' signed informed consent. Here we discuss our individual patients' problems through a series of inputs from the available global online community of experts with an aim to solve those patients' clinical problems with collective current best evidence-based information.
CASE REPORT
A 65 year old male patient, resident of Choutuppal, previously worked as a farmer who stopped working 2 years ago.
Date of History taking: 02/12/2022Date of Examination: 02/12/2022
CHEIF COMPLAINTS
- Shortness of breath since 6 days
HISTORY OF PRESENTING ILLNESS
The patient was apparently asymptomatic 25 years ago (that is when he was 40 years old), when he had cough, which was blood stained and was diagnosed with tuberculosis ( confirmatory test not known ) and was on ATT for 6 months after which he was relieved of his symptoms. Then 2 years ago he developed shortness of breath grade 2 ( unable to do ordinary activities ) which was insidious in onset and relieved temporarily on medication ( medication and dosage unknown ), from then he developed intermittent shortness of breath which was relieved on medication temporarily. 6 months ago he again developed shortness of breath ( grade 2 on walking 200-300 m ) which is insidious in onset, for which he was taken to higher healthcare centre where he was prescribed medications which he used irregularly. After that 5 months back he suffered from an accident where he fractured his left tibia and a left rib (managed with POP casting for 45 days). He experienced diffuse pain all over the abdomen 6 days ago which was insidious in onset and was not radiating.
H/O Jaundice, pruritus
NO H/O of Hematemesis, Malena, Vomiting, Nausea H/O bulky stools, black tarry, and clay-coloured.
NO H/O anorexia
NO H/O fever with chills
NO H/O blood transfusions
NO H/O tattoo marking
NO H/O loss of weight
NO H/O orthopnea, palpitations
NO H/O frothy urine
NO H/O haematuria, oliguria

Then recently 6 days ago he developed SOB insidious in onset ( grade 3). There is history of cough which is productive ( scanty quantity and mucoid, white in colour, no foreign bodies). 2 days back he developed diarrhoea, 8 stools on day 1, 10 on day 2.
H/O Jaundice, pruritus
NO H/O of Hematemesis, Malena, Vomiting, Nausea H/O bulky stools, black tarry, and clay-coloured.
NO H/O anorexia
NO H/O fever with chills
NO H/O blood transfusions
NO H/O tattoo marking
NO H/O loss of weight
NO H/O orthopnea, palpitations
NO H/O frothy urine
NO H/O haematuria, oliguria

Then recently 6 days ago he developed SOB insidious in onset ( grade 3). There is history of cough which is productive ( scanty quantity and mucoid, white in colour, no foreign bodies). 2 days back he developed diarrhoea, 8 stools on day 1, 10 on day 2.
PAST HISTORY
- History of pulmonary tuberculosis 25 years back- No history of DM
- No history of Hypertension, asthma, epilepsy, TB
- No history of prolonged hospital stay
- No history of previous surgeries
PERSONAL HISTORY
Appetite - Reduced since 1 year
Diet - Mixed
Bowel and Bladder - Regular
Sleep - inadequate
Addictions - stopped 20 years back, before alcohol and smoking
FAMILY HISTORY
None of the patient’s parents, siblings, or first-degree relatives have or have had similar complaints or any significant co-morbidities.
ALLERGIC HISTORY
No allergies to any kind of food or medication.
Asthma/ COPD/ CAD/ Blood transfusions
No surgeries, drug usage, allergies.
GENERAL EXAMINATION
Patient is conscious, coherent and cooperative, comfortably lying on the bed, well-oriented to time, place and person.
Pallor is present.




No Icterus, cyanosis, clubbing, generalised lymphadenopathy and no pedal oedema.
Pulse: Rate: 76 , rhythm (regular), character (normal), volume ( normal)
Peripheral pulsations [Carotid, brachial, radial, femoral, popliteal, posterior tibial, dorsalis pedis]- present
no radio radial delay
BP: 120/80 mm Hg measured on Right Upper arm in supine position
Respiratory Rate: 25 cpm
RESPIRATORY SYSTEM
INSPECTION:
1. Shape of Chest: normal
2. Tracheal position: central
3. Apical Impulse: not visible
4. Movements of the chest: Respiratory rate: 25cpm Type: abdominothoracic type no accessory muscles involved.
5. Skin over the chest: No engorged veins, sinuses, subcutaneous nodules, intercostal scars, or intercostal swellings.
6. All the areas appear normal.
PALPATION:
1. No local rise in temperature
2. No tenderness
3. All inspector findings confirmed. (Tracheal position, apex beat)
4. Expansion of the chest: equal in all planes
PERCUSSION:
Resonant all over the chest except infraxillary area
AUSCULTATION:
Normal breath sounds were heard in all areas except the left infra axillary where there are decreased breath sounds.
PER ABDOMEN
INSPECTION:

9 REGIONS
Shape: scaphoid
No Distention of Abdomen
Flanks: full
Umbilicus: normal
The skin over the abdomen: smooth
No engorged veins, visible pulsations, or hernia orifices.
PALPATION: no hepatomegaly no splenomegaly
PERCUSSION:
Normal
AUSCULTATION:
bowel sounds heard.
CVS
INSPECTION: Appears normal in shape, apex beat not visible
PALPATION: All inspectory findings are confirmed. Trachea is central No murmurs
AUSCULTATION S1, S2 heard
- No history of DM
- No history of Hypertension, asthma, epilepsy, TB
- No history of prolonged hospital stay
- No history of previous surgeries
PERSONAL HISTORY
Appetite - Reduced since 1 year
Diet - Mixed
Bowel and Bladder - Regular
Sleep - inadequate
Addictions - stopped 20 years back, before alcohol and smoking
FAMILY HISTORY
None of the patient’s parents, siblings, or first-degree relatives have or have had similar complaints or any significant co-morbidities.
ALLERGIC HISTORY
No allergies to any kind of food or medication.
Asthma/ COPD/ CAD/ Blood transfusions
No surgeries, drug usage, allergies.
GENERAL EXAMINATION
Patient is conscious, coherent and cooperative, comfortably lying on the bed, well-oriented to time, place and person.
Pallor is present.




No Icterus, cyanosis, clubbing, generalised lymphadenopathy and no pedal oedema.
Pulse: Rate: 76 , rhythm (regular), character (normal), volume ( normal)
Peripheral pulsations [Carotid, brachial, radial, femoral, popliteal, posterior tibial, dorsalis pedis]- present
no radio radial delay
BP: 120/80 mm Hg measured on Right Upper arm in supine position
Respiratory Rate: 25 cpm
RESPIRATORY SYSTEM
INSPECTION:
1. Shape of Chest: normal
2. Tracheal position: central
3. Apical Impulse: not visible
4. Movements of the chest: Respiratory rate: 25cpm Type: abdominothoracic type no accessory muscles involved.
5. Skin over the chest: No engorged veins, sinuses, subcutaneous nodules, intercostal scars, or intercostal swellings.
6. All the areas appear normal.
PALPATION:
1. No local rise in temperature
2. No tenderness
3. All inspector findings confirmed. (Tracheal position, apex beat)
4. Expansion of the chest: equal in all planes
PERCUSSION:
Resonant all over the chest except infraxillary area
AUSCULTATION:
Normal breath sounds were heard in all areas except the left infra axillary where there are decreased breath sounds.
PER ABDOMEN
INSPECTION:

9 REGIONS
Shape: scaphoid
No Distention of Abdomen
Flanks: full
Umbilicus: normal
The skin over the abdomen: smooth
No engorged veins, visible pulsations, or hernia orifices.
PALPATION: no hepatomegaly no splenomegaly
PERCUSSION:
Normal
AUSCULTATION:
bowel sounds heard.
PROVISIONAL DIAGNOSIS
Cor Pulmonale Heart failure with mid range preserved ejection fraction with anemia under evaluation with AKI on PCKD with a history of pulmonary TB 25 years back.


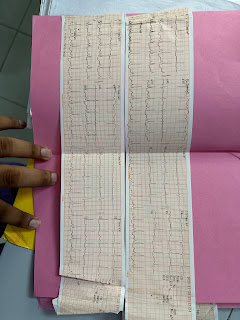
INVESTIGATIONS
29/11/2022


30/11/2022









02/12/2022






TREATMENT- LASIX 40 mg iv. bd- Neb. Salbutamol - fourth hourly fever chart - SpO2 monitoring - Augmentin 1.2 g iv stat



















Comments
Post a Comment